A situation most plants have faced at least once
It’s just after 9 in the morning. The first shift is in full swing. Machines are warmed up, supervisors are doing their rounds, and production targets are already being discussed.
Then it happens.
A contract worker near the furnace area suddenly feels dizzy and collapses. Someone shouts for help. Another person runs to call security. The line supervisor tries to remember where the first aid box is kept.
Someone asks loudly, “Doctor hai kya?”
Another replies, “Sunday ko visiting doctor aata hai.”
By the time a vehicle is arranged and the worker is moved out of the gate, twenty minutes are gone. The nearest hospital is still far. The HR manager’s phone starts ringing. EHS is alerted. By evening, reports begin circulating.
A few days later, during a routine visit, the Factory Inspector asks calmly:
“Aapka Occupational Health Centre kahan hai?”
Anyone who has worked inside an Indian plant knows this moment. It’s uncomfortable because it exposes gaps that everyone knew existed—but nobody addressed properly.
The real challenge industries are dealing with today
Most factories don’t ignore health and safety. That’s not the issue.
The issue is that many believe minimum arrangements are enough.
A few first aid boxes, a stretcher somewhere near the gate, a visiting doctor, and an ambulance number pinned to the notice board. On paper, it looks acceptable.
On the ground, it’s a different story.
Plants today are operating under pressure:
- Higher output with leaner manpower
- Large dependency on contract workers
- Hotter processes and longer shifts
- Workers ageing on the job
- Lifestyle diseases quietly increasing
- Audits becoming sharper and less forgiving
Health incidents are no longer treated as “unavoidable”. Every incident is questioned—by auditors, inspectors, clients, and sometimes courts.
In this environment, an Occupational Health Centre is no longer optional support.
It has become a risk control function, just like safety or maintenance.
What an Occupational Health Centre actually means in practice
Let’s move away from definitions.
In real industrial life, an OHC is not:
- Just a room with a bed
- A place where BP is checked occasionally
- A formality for inspections
A properly functioning OHC is where:
- Health risks are identified early
- Minor complaints are managed before escalation
- Occupational diseases are tracked over years
- Emergencies are stabilised, not panicked over
- Documentation protects both worker and management
When an OHC works well, nobody talks about it.
When it doesn’t, it becomes the centre of every discussion—usually after something has gone wrong.
How an OHC actually functions day to day
1. Most of the work is quiet and routine
People imagine emergencies when they think of OHCs. In reality, emergencies are rare.
What fills most OHC registers are everyday issues:
- Persistent headaches from heat exposure
- Back pain from improper lifting
- Acidity and fatigue during night shifts
- Minor cuts that can get infected
- BP spikes in senior operators
- Sugar fluctuations in drivers and supervisors
If these are handled early, they never become incidents.
If ignored, they turn into absenteeism, accidents, or compensation cases.
A good OHC quietly absorbs these pressures.
2. Occupational diseases creep in slowly
Very few occupational illnesses show dramatic symptoms.
Noise-induced hearing loss.
Dust-related lung changes.
Chemical skin conditions.
They develop over years.
I’ve seen plants where:
- Audiometry tests were done every year but never compared
- Spirometry values declined slowly, unnoticed
- Workers kept rotating jobs without health trend tracking
The reports were filed. Compliance looked perfect.
The damage continued silently.
An OHC is supposed to be the place where medical data is interpreted, not just stored.
3. Emergency readiness is revealed only once
Emergency systems always look good during audits.
Real emergencies are messy.
People panic. Phones ring. Roles blur. Decisions get delayed.
In those moments, only a trained, confident OHC team makes a difference.
Simple questions decide outcomes:
- Who reaches the patient first?
- Who gives oxygen correctly?
- Is the referral hospital already informed?
- Are papers ready if police or inspector arrive?
Preparation doesn’t show until the day it’s needed.
Setting up an OHC – how it actually works on the ground
This is where many organisations struggle—not due to lack of money, but lack of clarity.
Step 1: Know your risk, honestly
Before planning anything, stop and assess:
- What are the actual hazards in your plant?
- How many people work per shift, including contractors?
- How far is the nearest emergency hospital in real traffic conditions?
- What incidents have already happened in the past?
An OHC for a cement plant cannot be copied from an IT park.
Risk profile should decide everything.
Step 2: Choose location with emergencies in mind
A common mistake is placing the OHC near admin offices because it “looks neat”.
In emergencies, neat doesn’t matter. Access does.
The OHC should be:
- Easy to reach from production areas
- Accessible by ambulance without obstruction
- Clearly marked
- Close enough to the gate for quick referral
When someone collapses, no one wants to run across the plant.
Step 3: Staffing is about experience, not just degrees
Staffing patterns vary by manpower strength, but one thing stays constant:
Industrial exposure matters.
Doctors and nurses who have only worked in hospitals often struggle initially in plants. Industrial health is a different environment altogether.
An effective OHC team usually includes:
- A doctor comfortable with occupational hazards
- A nurse who understands shift realities
- A pharmacist who controls medicines and records
- Trained first aiders on shop floor
The team must understand the plant—not just medicine.
Step 4: Equipment must be usable, not ornamental
Many OHCs look impressive but fail basic tests.
I’ve personally seen:
- Oxygen cylinders found empty during checks
- ECG machines never switched on
- Emergency drugs expired months ago
Equipment should be:
- Relevant to plant risks
- Maintained regularly
- Known to staff
Unused equipment is as bad as no equipment.
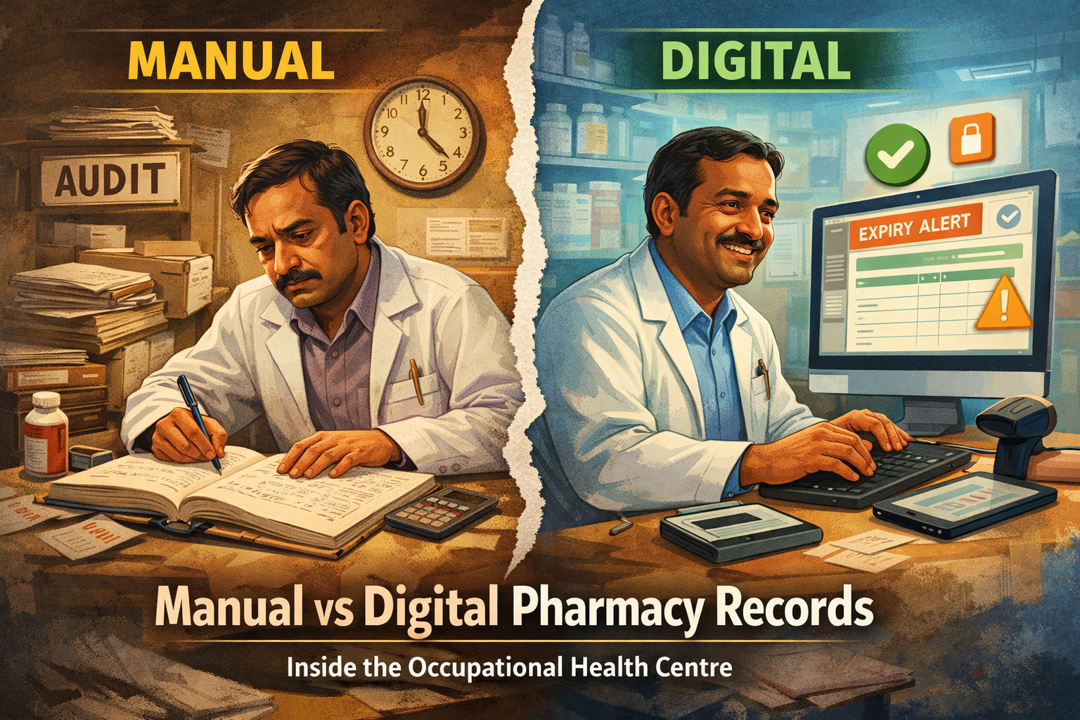
Step 5: Medicine management needs discipline
This is where strong OHCs separate themselves from weak ones.
Without proper systems:
- Medicines expire unnoticed
- Emergency drugs go missing
- Indents become irregular
- Cold-chain products lose efficacy
A structured inventory system—preferably managed by a trained pharmacist—keeps the OHC audit-ready and clinically safe.
Legal and compliance reality in India
The Factories Act is still central
Under the Factories Act and respective State Factory Rules:
- OHCs are mandatory beyond defined manpower limits
- Medical surveillance is compulsory for hazardous processes
- Records must be maintained and produced when demanded
Inspectors today don’t just tick boxes.
They ask practical questions. They observe functionality.
Other compliance pressures
Beyond the Factories Act, OHCs are evaluated during:
- ISO 45001 audits
- Client safety audits
- Corporate EHS reviews
- Insurance inspections
Often, the OHC becomes the face of the organisation during these visits.
Mistakes industries repeatedly make
After years in the field, certain patterns are impossible to ignore.
Some of the most common ones:
Treating OHC purely as an expense.
Outsourcing everything and never reviewing performance.
Ignoring contract workers’ health tracking.
Collecting reports but never analysing them.
Keeping OHC disconnected from EHS and HR.
Never discussing health data in management meetings.
None of these fail immediately.
They fail slowly—and then suddenly.
Cost, risk, and compliance – the real balance
Management often asks one question first:
“Kitna kharcha aayega?”
A better question is:
“What will it cost if something serious happens?”
One serious incident can lead to:
- Compensation claims
- Legal proceedings
- Production stoppage
- Media scrutiny
- Loss of client trust
A well-managed OHC quietly reduces these risks every single day.
A practical checklist that actually helps
If you want a quick reality check, ask these questions:
- Is the OHC accessible during all shifts?
- Are emergency drugs checked weekly?
- Are occupational health reports reviewed, not just filed?
- Do contract workers receive the same medical attention?
- Is there a clear referral protocol?
- Are mock drills involving OHC conducted?
- Does management review health trends periodically?
If answers are uncertain, improvement is needed.
Where Occupational Health Centres are heading
Across Indian industries, changes are visible:
- Gradual shift to digital medical records
- Better use of health trend data
- Closer integration of health with safety
- Growing focus on mental well-being
- Stronger role of pharmacists and nurses in operations
The future OHC will not be flashy.
It will be quiet, efficient, data-aware, and deeply practical.